Blue Circle
Medi Services


What is schizophrenia?
Schizophrenia is a brain disorder that affects the way a person behaves, thinks, and sees the world. People with schizophrenia often have an altered perception of reality. They may see or hear things that don’t exist, speak in strange or confusing ways, believe that others are trying to harm them, or feel like they’re being constantly watched. This can make it difficult to negotiate the activities of daily life, and people with schizophrenia may withdraw from the outside world or act out in confusion and fear.
Although schizophrenia is a chronic disorder, there is help available. With support, medication, and therapy, many people with schizophrenia are able to function independently and live fulfilling lives.Early warning signs of schizophrenia
In some people, schizophrenia appears suddenly
and without warning. But for most, it comes on slowly, with subtle warning
signs and a gradual decline in functioning long before the first severe
episode. Many friends and family members of people with schizophrenia report
knowing early on that something was wrong with their loved one, they just
didn’t know what.
In this early phase, people with schizophrenia
often seem eccentric, unmotivated, emotionless, and reclusive. They isolate
themselves, start neglecting their appearance, say peculiar things, and show a
general indifference to life. They may abandon hobbies and activities, and
their performance at work or school deteriorates.
The most common early warning signs of schizophrenia include:
- Social
withdrawal
- Hostility
or suspiciousness
- Deterioration
of personal hygiene
- Flat,
expressionless gaze
- Inability
to cry or express joy
- Inappropriate
laughter or crying
- Depression
- Oversleeping
or insomnia
- Odd
or irrational statements
- Forgetful;
unable to concentrate
- Extreme
reaction to criticism
- Strange
use of words or way of speaking
While these warning signs can result from a
number of problems—not just schizophrenia—they are cause for concern. When
out-of-the-ordinary behavior is causing problems in your life or the life of a
loved one, seek medical advice. If schizophrenia or another mental problem is
the cause, treatment will help.
There are five types of symptoms
characteristic of schizophrenia: delusions, hallucinations, disorganized
speech, disorganized behavior, and the so-called “negative” symptoms. However,
the signs and symptoms of schizophrenia vary dramatically from person to
person, both in pattern and severity. Not every person with schizophrenia will
have all symptoms, and the symptoms of schizophrenia may also change over time.
Delusions
A delusion is a firmly-held idea that a person
has despite clear and obvious evidence that it isn’t true. Delusions are
extremely common in schizophrenia, occurring in more than 90% of those who have
the disorder. Often, these delusions involve illogical or bizarre ideas or
fantasies. Common schizophrenic delusions include:
- Delusions of persecution – Belief that
others, often a vague “they,” are out to get him or her. These persecutory
delusions often involve bizarre ideas and plots (e.g. “Martians are trying
to poison me with radioactive particles delivered through my tap water”).
- Delusions of reference – A neutral
environmental event is believed to have a special and personal meaning.
For example, a person with schizophrenia might believe a billboard or a
person on TV is sending a message meant specifically for them.
- Delusions of grandeur – Belief that
one is a famous or important figure, such as Jesus Christ or Napolean.
Alternately, delusions of grandeur may involve the belief that one has
unusual powers that no one else has (e.g. the ability to fly).
- Delusions of control – Belief that
one’s thoughts or actions are being controlled by outside, alien forces.
Common delusions of control include thought broadcasting (“My private
thoughts are being transmitted to others”), thought insertion (“Someone is
planting thoughts in my head”), and thought withdrawal (“The CIA is
robbing me of my thoughts”).
Hallucinations
Hallucinations are sounds or other sensations
experienced as real when they exist only in the person's mind. While
hallucinations can involve any of the five senses, auditory hallucinations
(e.g. hearing voices or some other sound) are most common in schizophrenia.
Visual hallucinations are also relatively common. Research suggests that
auditory hallucinations occur when people misinterpret their own inner
self-talk as coming from an outside source.
Schizophrenic hallucinations are usually
meaningful to the person experiencing them. Many times, the voices are those of
someone they know. Most commonly, the voices are critical, vulgar, or abusive.
Hallucinations also tend to be worse when the person is alone.
Disorganized speech
Fragmented thinking is characteristic of
schizophrenia. Externally, it can be observed in the way a person speaks.
People with schizophrenia tend to have trouble concentrating and maintaining a
train of thought. They may respond to queries with an unrelated answer, start
sentences with one topic and end somewhere completely different, speak
incoherently, or say illogical things.
Common signs of disorganized speech in
schizophrenia include:
- Loose associations – Rapidly
shifting from topic to topic, with no connection between one thought and
the next.
- Neologisms – Made-up words
or phrases that only have meaning to the patient.
- Perseveration – Repetition of
words and statements; saying the same thing over and over.
- Clang – Meaningless
use of rhyming words (“I said the bread and read the shed and fed Ned at
the head").
Disorganized behavior
Schizophrenia disrupts goal-directed activity,
causing impairments in a person’s ability to take care of him or herself, work,
and interact with others. Disorganized behavior appears as:
- A
decline in overall daily functioning
- Unpredictable
or inappropriate emotional responses
- Behaviors
that appear bizarre and have no purpose
- Lack
of inhibition and impulse control
Negative symptoms (absence of normal behaviors)
The so-called “negative” symptoms of
schizophrenia refer to the absence of normal behaviors found in healthy
individuals. Common negative symptoms of schizophrenia include:
- Lack of emotional expression – Inexpressive
face, including a flat voice, lack of eye contact, and blank or restricted
facial expressions.
- Lack of interest or enthusiasm – Problems with
motivation; lack of self-care.
- Seeming lack of interest in the
world –
Apparent unawareness of the environment; social withdrawal.
- Speech difficulties and
abnormalities – Inability to carry a
conversation; short and sometimes disconnected replies to questions;
speaking in monotone.
The causes of schizophrenia are not fully
known. However, it appears that schizophrenia usually results from a complex
interaction between genetic and environmental factors.
Genetic causes of schizophrenia
Schizophrenia has a strong hereditary
component. Individuals with a first-degree relative (parent or sibling) who has
schizophrenia have a 10 percent chance of developing the disorder, as opposed
to the one percent chance of the general population.
But schizophrenia is only influenced by
genetics, not determined by it. While schizophrenia runs in families, about 60%
of schizophrenics have no family members with the disorder. Furthermore,
individuals who are genetically predisposed to schizophrenia don’t always
develop the disease, which shows that biology is not destiny.
Environmental causes of schizophrenia
Twin and adoption studies suggest that
inherited genes make a person vulnerable to schizophrenia and then
environmental factors act on this vulnerability to trigger the disorder.
As for the environmental factors involved,
more and more research is pointing to stress, either during pregnancy or at a
later stage of development. High levels of stress are believed to trigger
schizophrenia by increasing the body’s production of the hormone cortisol.
Research points to several stress-inducing
environmental factors that may be involved in schizophrenia, including:
- Prenatal
exposure to a viral infection
- Low
oxygen levels during birth (from prolonged labor or premature birth)
- Exposure
to a virus during infancy
- Early
parental loss or separation
- Physical
or sexual abuse in childhood
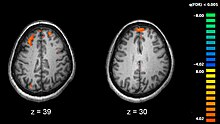
Abnormal brain structure
In addition to abnormal brain chemistry,
abnormalities in brain structure may also play a role in schizophrenia.
Enlarged brain ventricles are seen in some schizophrenics, indicating a deficit
in the volume of brain tissue. There is also evidence of abnormally low
activity in the frontal lobe, the area of the brain responsible for planning,
reasoning, and decision-making.
Some studies also suggest that abnormalities
in the temporal lobes, hippocampus, and amygdala are connected to
schizophrenia’s positive symptoms. But despite the evidence of brain
abnormalities, it is highly unlikely that schizophrenia is the result of any
one problem in any one region of the brain.
When the signs and symptoms of schizophrenia
are ignored or improperly treated, the effects can be devastating, both to the
individual with the disorder and those around him or her. Some of the possible
effects of schizophrenia are:
- Relationship problems. Relationships
suffer because people with schizophrenia often withdraw and isolate
themselves. Paranoia can also cause a person with schizophrenia to be
suspicious of friends and family.
- Disruption to normal daily
activities. Schizophrenia
causes significant disruptions to daily functioning, both because of
social difficulties and because everyday tasks become hard, if not
impossible to do. A schizophrenic person’s delusions, hallucinations, and
disorganized thoughts typically prevent him or her from doing normal
things like bathing, eating, or running errands.
- Alcohol and drug abuse. People with
schizophrenia frequently develop problems with alcohol ordrugs, which are often used in an
attempt to self-medicate, or relieve symptoms. In addition, they may also
be heavy smokers, a complicating situation as cigarette smoke can
interfere with the effectiveness of medications prescribed for the
disorder.
- Increased suicide risk. People with
schizophrenia have a high risk of attempting suicide. Any suicidal talk, threats,
or gestures should be taken very seriously. People with schizophrenia are
especially likely to commit suicide during psychotic episodes, during
periods of depression, and in the first six months after they’ve started
treatment.
A diagnosis of schizophrenia is made based on
a full psychiatric evaluation, medical history, physical exam, and lab tests.
- Psychiatric evaluation – The doctor or
psychiatrist will ask a series of questions about you or your loved one's
symptoms, psychiatric history, and family history of mental health
problems.
- Medical history and exam – Your doctor
will ask about your personal and family health history. He or she will
also perform a complete physical examination to check for medical issues
that could be causing or contributing to the problem.
- Laboratory tests – While there
are no laboratory tests that can diagnose schizophrenia, simple blood and
urine tests can rule out other medical causes of symptoms. The doctor may
also order brain-imaging studies, such as an MRI or a CT scan, in order to
look for brain abnormalities associated with schizophrenia.
Criteria to diagnose schizophrenia
- The presence of two or more of the
following symptoms for at least 30 days:
1. Hallucinations
2. Delusions
3. Disorganized
speech
4. Disorganized
or catatonic behavior
5. Negative
symptoms (emotional flatness, apathy, lack of speech)
- Significant problems functioning at work or
school, relating to other people, and taking care of oneself.
- Continuous signs of schizophrenia for at least six
months, with active symptoms (hallucinations, delusions, etc.) for at
least one month.
- No other mental health disorder,
medical issue, or substance abuse problem is causing the symptoms.
The medical and psychological conditions the
doctor must rule out before diagnosing schizophrenia include:
- Other psychotic disorders – Schizophrenia
is a type of psychotic disorder, meaning it involves a significant loss of
contact with reality. But there are other psychotic disorders that cause
similar symptoms of psychosis, including schizoaffective disorder,
schizophreniform disorder, and brief psychotic disorder. Because of the
difficulty in differentiating between the psychotic disorders, it may take
six months or longer to arrive at a correct diagnosis.
- Substance abuse – Psychotic
symptoms can be triggered by many drugs, including alcohol, PCP, heroin,
amphetamines, and cocaine. Some over-the-counter and prescription drugs
can also trigger psychotic reactions. A toxicology screen can rule out
drug-induced psychosis. If substance abuse is involved, the physician will
determine whether the drug is the source of the symptoms or merely an
aggravating factor.
- Medical conditions –
Schizophrenia-like symptoms can also result from certain neurological
disorders (such as epilepsy, brain tumors, and encephalitis), endocrine
and metabolic disturbances, and autoimmune conditions involving the
central nervous system.
- Mood disorders – Schizophrenia
often involves changes in mood, including mania and depression. While
these mood changes are typically less severe than those seen in bipolar
disorder and major depressive disorder, they can make diagnosis tricky.
Schizophrenia is particularly difficult to distinguish from bipolar
disorder. The positive symptoms of schizophrenia (delusions, hallucinations,
and disorganized speech) can look like a manic episode of bipolar
disorder, while the negative symptoms of schizophrenia (apathy, social
withdrawal, and low energy) can look like a depressive episode.
- Post-traumatic stress disorder
(PTSD) – PTSD is an
anxiety disorder that can develop after exposure to a traumatic event,
such as military combat, an accident, or a violent assault. People with
PTSD experience symptoms that are similar to schizophrenia. The images,
sounds, and smells of PTSD flashbacks can look like psychotic
hallucinations. The PTSD symptoms of emotional numbness and avoidance can
look like the negative symptoms of schizophrenia.
With proper treatment, patients can lead productive lives - according to the National Institute of Mental Health1 (NIMN), treatment can help relieve many of the symptoms of schizophrenia. However, the majority of patients with the disorder have to cope with the symptoms for life. This does not mean that a person with schizophrenia who receives treatment cannot lead a rewarding, productive and meaningful life in his or her community.
Schizophrenia most commonly strikes between the ages of 15 to 25 among men, and about 25 to 35 in women. In many cases the disorder develops so slowly that the sufferer does not know he/she has it for a long time. While, with other people it can strike suddenly and develop fast.
Schizophrenia, possibly many illnesses combined - it is a complex, chronic, severe, and disabling brain disorder and affects approximately 1% of all adults globally. Experts say schizophrenia is probably many illnesses masquerading as one. Research indicates that schizophrenia is likely to be the result of faulty neuronal development in the brain of the fetus, which later in life emerges as a full-blown illness.
The brain
Our brain consists of billions of nerve cells. Each nerve cell has branches that give out and receive messages from other nerve cells.
The ending of these nerve cells release neurotransmitters - types of chemicals. These neurotransmitters carry messages from the endings of one nerve cell to the nerve cell body of another. In the brain of a person who has schizophrenia, this messaging system does not work properly.
Symptoms of schizophrenia
There is, to date, no physical or laboratory test that can absolutely diagnose schizophrenia. The doctor, a psychiatrist, will make a diagnosis based on the patient's clinical symptoms. However, physical testing can rule out some other disorders and conditions which sometimes have similar symptoms, such as seizure disorders, thyroid dysfunction, braintumor, drug use, and metabolic disorders.
Symptoms and signs of schizophrenia will vary, depending on the individual. The symptoms are classified into four categories:
- Positive symptoms - also known as psychotic symptoms. These are symptoms that appear, which people without schizophrenia do not have. For example, delusion.
- Negative symptoms - these refer to elements that are taken away from the individual; loss or absence of normal traits or abilities that people without schizophrenia normally have. For example, blunted emotion.
- Cognitive symptoms - these are symptoms within the person's thought processes. They may be positive or negative symptoms, for example, poor concentration is a negative symptom.
- Emotional symptoms - these are symptoms within the person's feelings. They are usually negative symptoms, such as blunted emotions.
Below is a list of the major symptoms:
- Delusions - The patient has false beliefs of persecution, guilt of grandeur. He/she may feel things are being controlled from outside. It is not uncommon for people with schizophrenia to describe plots against them. They may think they have extraordinary powers and gifts. Some patients with schizophrenia may hide in order to protect themselves from an imagined persecution.
- Hallucinations - hearing voices is much more common than seeing, feeling, tasting, or smelling things which are not there, but seem very real to the patient.
- Thought disorder - the person may jump from one subject to another for no logical reason. The speaker may be hard to follow. The patient's speech might be muddled and incoherent. In some cases the patient may believe that somebody is messing with his/her mind.
Other symptoms schizophrenia patients may experience include:
- Lack of motivation (avolition) - the patient loses his/her drive. Everyday automatic actions, such as washing and cooking are abandoned. It is important that those close to the patient understand that this loss of drive is due to the illness, and has nothing to do with slothfulness.
- Poor expression of emotions - responses to happy or sad occasions may be lacking, or inappropriate.
- Social withdrawal - when a patient with schizophrenia withdraws socially it is often because he/she believes somebody is going to harm them. Other reasons could be a fear of interacting with other humans because of poor social skills.
- Unaware of illness - as the hallucinations and delusions seem so real for the patients, many of them may not believe they are ill. They may refuse to take medications which could help them enormously for fear of side-effects, for example.
- Cognitive difficulties - the patient's ability to concentrate, remember things, plan ahead, and to organize himself/herself are affected. Communication becomes more difficult.Individuals with schizophrenia may experience hallucinations (most reported are hearing voices), delusions (often bizarre or persecutory in nature), and disorganized thinking and speech. The last may range from loss of train of thought, to sentences only loosely connected in meaning, to speech that is not understandable known as word salad. Social withdrawal, sloppiness of dress and hygiene, and loss of motivation and judgment are all common in schizophrenia.[17] There is often an observable pattern of emotional difficulty, for example lack of responsiveness.[18] Impairment in social cognition is associated with schizophrenia,[19] as are symptoms of paranoia. Social isolation commonly occurs.[20] Difficulties in working and long-term memory, attention, executive functioning, and speed ofprocessing also commonly occur.[11] In one uncommon subtype, the person may be largely mute, remain motionless in bizarre postures, or exhibit purposeless agitation, all signs of catatonia.[21] About 30 to 50 percent of people with schizophrenia fail to accept that they have an illness or comply with their recommended treatment.[22] Treatment may have some effect on insight.[23] People with schizophrenia often find facial emotion perception to be difficult.[24]
People with schizophrenia may have a high rate of irritable bowel syndrome but they often do not mention it unless specifically asked.[25]
Positive and negative
Schizophrenia is often described in terms of positive and negative (or deficit) symptoms.[26] Positive symptoms are those that most individuals do not normally experience but are present in people with schizophrenia. They can include delusions, disordered thoughts and speech, and tactile, auditory, visual, olfactory andgustatory hallucinations, typically regarded as manifestations of psychosis.[27] Hallucinations are also typically related to the content of the delusional theme.[28]Positive symptoms generally respond well to medication.[28]
Negative symptoms are deficits of normal emotional responses or of other thought processes, and are less responsive to medication.[17] They commonly include flat expressions or little emotion, poverty of speech, inability to experience pleasure, lack of desire to form relationships, and lack of motivation. Negative symptoms appear to contribute more to poor quality of life, functional ability, and the burden on others than do positive symptoms.[29] People with greater negative symptoms often have a history of poor adjustment before the onset of illness, and response to medication is often limited.[17][30]
Cognitive dysfunction
Deficits in cognitive abilities are widely recognized as a core feature of schizophrenia.[31][32][33] The extent of the cognitive deficits an individual experiences is a predictor of how functional an individual will be, the quality of occupational performance, and how successful the individual will be in maintaining treatment.[34] The presence and degree of cognitive dysfunction in individuals with schizophrenia has been reported to be a better indicator of functionality than the presentation of positive or negative symptoms.[31] The deficits impacting the cognitive function are found in a large number of areas: working memory, long-term memory,[35][36]verbal declarative memory,[37] semantic processing,[38] episodic memory,[34] attention, learning (particularly verbal learning).[35] Deficits in verbal memory are the most pronounced in individuals with schizophrenia, and are not accounted for by deficit in attention. Verbal memory impairment has been linked to a decreased ability in individuals with schizophrenia to semantically encode (process information relating to meaning), which is cited as a cause for another known deficit in long-term memory.[35] When given a list of words, healthy individuals remember positive words more frequently (known as the Pollyanna principle ); however, individuals with schizophrenia tend to remember all words equally regardless of their connotations, suggesting that the experience of anhedonia impairs the semantic encoding of the words.[35] These deficits have been found in individuals before the onset of the illness to some extent.[31][33][39] First-degree family members of individuals with schizophrenia and other high-risk individuals also show a degree of deficit in cognitive abilities, and specifically in working memory.[39] A review of the literature on cognitive deficits in individuals with schizophrenia shows that the deficits may be present in early adolescence, or as early as childhood.[31] The deficits which an individual with schizophrenia presents tend to remain the same over time in most patients, or follow an identifiable course based upon environmental variables.[31][35]
Although the evidence that cognitive deficits remain stable over time is reliable and abundant,[34][35] much of the research in this domain focuses on methods to improve attention and working memory[35][36] Efforts to improve learning ability in individuals with schizophrenia using a high- versus low-reward condition and an instruction-absent or instruction-present condition revealed that increasing reward leads to poorer performance while providing instruction leads to improved performance, highlighting that some treatments may exist to increase cognitive performance.[35] Training individuals with schizophrenia to alter their thinking, attention, and language behaviors by verbalizing tasks, engaging in cognitive rehearsal, giving self-instructions, giving coping statements to the self to handle failure, and providing self-reinforcement for success, significantly improves performance on recall tasks.[35] This type of training, known as self-instructional (SI) training, produced benefits such as lower number of nonsense verbalizations and improved recall while distracted.[35]
Onset
Late adolescence and early adulthood are peak periods for the onset of schizophrenia,[11] critical years in a young adult's social and vocational development.[40] In 40% of men and 23% of women diagnosed with schizophrenia, the condition manifested itself before the age of 19.[41] To minimize the developmental disruption associated with schizophrenia, much work has recently been done to identify and treat the prodromal (pre-onset) phase of the illness, which has been detected up to 30 months before the onset of symptoms.[40] Those who go on to develop schizophrenia may experience transient or self-limiting psychotic symptoms[42] and the non-specific symptoms of social withdrawal, irritability, dysphoria,[43] and clumsiness[44] during the prodromal phase.Causes
A combination of genetic and environmental factors play a role in the development of schizophrenia.[8][11] People with a family history of schizophrenia who have a transient psychosis have a 20–40% chance of being diagnosed one year later.[45]Genetic
Estimates of heritability vary because of the difficulty in separating the effects of genetics and the environment;[46] averages of 0.80 have been given.[47] The greatest risk for developing schizophrenia is having a first-degree relative with the disease (risk is 6.5%); more than 40% of monozygotic twins of those with schizophrenia are also affected.[8] If one parent is affected the risk is about 13% and if both are affected the risk is nearly 50%.[47]
Many genes are believed to be involved in schizophrenia, each of small effect and unknown transmission and expression.[8] Many possible candidates have been proposed, including specific copy number variations, NOTCH4, and histone protein loci.[48] A number of genome-wide associations such as zinc finger protein 804A have also been linked.[49] There appears to be overlap in the genetics of schizophrenia and bipolar disorder.[50] Evidence is emerging that the genetic architecture of schizophrenia involved both common and rare risk variation.[51]
Assuming a hereditary basis, one question from evolutionary psychology is why genes that increase the likelihood of psychosis evolved, assuming the condition would have been maladaptive from an evolutionary point of view. One idea is that genes are involved in the evolution of language and human nature, but to date such ideas remain little more than hypothetical in nature.[52][53]
Causes
A combination of genetic and environmental factors play a role in the development of schizophrenia.[8][11] People with a family history of schizophrenia who have a transient psychosis have a 20–40% chance of being diagnosed one year later.[45]Genetic
Estimates of heritability vary because of the difficulty in separating the effects of genetics and the environment;[46] averages of 0.80 have been given.[47] The greatest risk for developing schizophrenia is having a first-degree relative with the disease (risk is 6.5%); more than 40% of monozygotic twins of those with schizophrenia are also affected.[8] If one parent is affected the risk is about 13% and if both are affected the risk is nearly 50%.[47]
Many genes are believed to be involved in schizophrenia, each of small effect and unknown transmission and expression.[8] Many possible candidates have been proposed, including specific copy number variations, NOTCH4, and histone protein loci.[48] A number of genome-wide associations such as zinc finger protein 804A have also been linked.[49] There appears to be overlap in the genetics of schizophrenia and bipolar disorder.[50] Evidence is emerging that the genetic architecture of schizophrenia involved both common and rare risk variation.[51]
Assuming a hereditary basis, one question from evolutionary psychology is why genes that increase the likelihood of psychosis evolved, assuming the condition would have been maladaptive from an evolutionary point of view. One idea is that genes are involved in the evolution of language and human nature, but to date such ideas remain little more than hypothetical in nature.[52][53]
Environment
Environmental factors associated with the development of schizophrenia include the living environment, drug use, and prenatal stressors.[11]
Parenting style seems to have no major effect, although people with supportive parents do better than those with critical or hostile parents.[8] Childhood trauma, death of a parent, and being bullied or abused increase the risk of psychosis.[54] Living in an urban environment during childhood or as an adult has consistently been found to increase the risk of schizophrenia by a factor of two,[8][11] even after taking into account drug use, ethnic group, and size of social group.[55] Other factors that play an important role include social isolation and immigration related to social adversity, racial discrimination, family dysfunction, unemployment, and poor housing conditions.[8][56]
It has been hypothesised that in some people, development of schizophrenia is related to intestinal tract dysfunction such as seen with non-celiac gluten sensitivity or abnormalities in the intestinal flora.[57]A subgroup of persons with schizophrenia present an immune response to gluten different from that found in people with celiac, with elevated levels of certain serum biomarkers of gluten sensitivity such as anti-gliadin IgG or anti-gliadin IgA antibodies.[58]
Substance use
About half of those with schizophrenia use drugs or alcohol excessively.[59] Amphetamine, cocaine, and to a lesser extent alcohol, can result in a transient stimulant psychosis or alcohol-related psychosisthat presents very similarly to schizophrenia.[8][60] Although it is not generally believed to be a cause of the illness, people with schizophrenia use nicotine at much higher rates than the general population.[61]
Alcohol abuse can occasionally cause the development of a chronic, substance-induced psychotic disorder via a kindling mechanism.[62] Alcohol use is not associated with an earlier onset of psychosis.[63]
Cannabis can be a contributory factor in schizophrenia,[7][64][65] potentially causing the disease in those who are already at risk.[65] The increased risk may require the presence of certain genes within an individual[65] or may be related to preexisting psychopathology.[7] Early exposure is strongly associated with an increased risk.[7] The size of the increased risk is not clear,[66] but appears to be in the range of two to three times greater for psychosis.[64] Higher dosage and greater frequency of use are indicators of increased risk of chronic psychoses.[64]
Other drugs may be used only as coping mechanisms by individuals who have schizophrenia, to deal with depression, anxiety, boredom, and loneliness.[59][67]
Developmental factors
Factors such as hypoxia and infection, or stress and malnutrition in the mother during fetal development, may result in a slight increase in the risk of schizophrenia later in life.[11] People diagnosed with schizophrenia are more likely to have been born in winter or spring (at least in the northern hemisphere), which may be a result of increased rates of viral exposures in utero.[8] The increased risk is about five to eight percent.[68] Other infections during pregnancy or around the time of birth that may increase the risk include Toxoplasma gondi and Chlamydia.[69]
Mechanisms
A number of attempts have been made to explain the link between altered brain function and schizophrenia.[11] One of the most common is the dopamine hypothesis, which attributes psychosis to the mind's faulty interpretation of the misfiring of dopaminergic neurons.[11]Psychological
Many psychological mechanisms have been implicated in the development and maintenance of schizophrenia. Cognitive biases have been identified in those with the diagnosis or those at risk, especially when under stress or in confusing situations.[70] Some cognitive features may reflect global neurocognitive deficits such as memory loss, while others may be related to particular issues and experiences.[71][72]
Despite a demonstrated appearance of blunted affect, recent findings indicate that many individuals diagnosed with schizophrenia are emotionally responsive, particularly to stressful or negative stimuli, and that such sensitivity may cause vulnerability to symptoms or to the disorder.[73][74] Some evidence suggests that the content of delusional beliefs and psychotic experiences can reflect emotional causes of the disorder, and that how a person interprets such experiences can influence symptomatology.[75][76][77] The use of "safety behaviors" (acts such as gestures or the use of words in specific contexts) to avoid or neutralize imagined threats may actually contribute to the chronicity of delusions.[78] Further evidence for the role of psychological mechanisms comes from the effects ofpsychotherapies on symptoms of schizophrenia.[79]
Neurological

Schizophrenia is associated with subtle differences in brain structures, found in forty to fifty percent of cases, and in brain chemistry during acute psychotic states.[11] Studies using neuropsychological tests and brain imaging technologies such as fMRI and PET to examine functional differences in brain activity have shown that differences seem to occur most commonly in the frontal lobes, hippocampus and temporal lobes.[80] Reductions in brain volume, smaller than those found in Alzheimer's disease, have been reported in areas of the frontal cortex and temporal lobes. It is uncertain whether these volumetric changes are progressive or exist prior to the onset of the disease.[44] These differences have been linked to the neurocognitive deficits often associated with schizophrenia.[81] Because neural circuits are altered, it has alternatively been suggested that schizophrenia should be thought of as a collection of neurodevelopmental disorders.[82] There has been debate on whether treatment with antipsychotics can itself cause reduction of brain volume.[83]
Particular attention has been paid to the function of dopamine in the mesolimbic pathway of the brain. This focus largely resulted from the accidental finding thatphenothiazine drugs, which block dopamine function, could reduce psychotic symptoms. It is also supported by the fact that amphetamines, which trigger the release of dopamine, may exacerbate the psychotic symptoms in schizophrenia.[84] The influential dopamine hypothesis of schizophrenia proposed that excessive activation of D2 receptors was the cause of (the positive symptoms of) schizophrenia. Although postulated for about 20 years based on the D2 blockade effect common to all antipsychotics, it was not until the mid-1990s that PET and SPET imaging studies provided supporting evidence. The dopamine hypothesis is now thought to be simplistic, partly because newer antipsychotic medication (atypical antipsychotic medication) can be just as effective as older medication (typical antipsychotic medication), but also affects serotonin function and may have slightly less of a dopamine blocking effect.[85]
Interest has also focused on the neurotransmitter glutamate and the reduced function of the NMDA glutamate receptor in schizophrenia, largely because of the abnormally low levels of glutamate receptors found in the postmortem brains of those diagnosed with schizophrenia,[86] and the discovery that glutamate-blocking drugs such as phencyclidine and ketamine can mimic the symptoms and cognitive problems associated with the condition.[87] Reduced glutamate function is linked to poor performance on tests requiring frontal lobe and hippocampal function, and glutamate can affect dopamine function, both of which have been implicated in schizophrenia; this has suggested an important mediating (and possibly causal) role of glutamate pathways in the condition.[88] But positive symptoms fail to respond to glutamatergic medication.[89]
Diagnosis
Subtype classifications – such as catatonic and paranoid schizophrenia – are removed. These were retained in previous revisions largely for reasons of tradition, but had subsequently proved to be of little worth.[91]- Catatonia is no longer so strongly associated with schizophrenia.[92]
- In describing a person's schizophrenia, it is recommended that a better distinction be made between the current state of the condition and its historical progress, to achieve a clearer overall characterization.[91]
- Special treatment of Schneider's first-rank symptoms is no longer recommended.[91]
- Schizoaffective disorder is better defined to demarcate it more cleanly from schizophrenia.[91]
- An assessment covering eight domains of psychopathology – such as whether hallucination or mania is experienced – is recommended to help clinical decision-making.[93]
The ICD-10 criteria are typically used in European countries, while the DSM criteria are used in the United States and to varying degrees around the world, and are prevailing in research studies. The ICD-10 criteria put more emphasis on Schneiderian first-rank symptoms. In practice, agreement between the two systems is high.[94]
If signs of disturbance are present for more than a month but less than six months, the diagnosis of schizophreniform disorder is applied. Psychotic symptoms lasting less than a month may be diagnosed as brief psychotic disorder, and various conditions may be classed as psychotic disorder not otherwise specified, while schizoaffective disorder is diagnosed if symptoms of mood disorder are substantially present alongside psychotic symptoms. If the psychotic symptoms are the direct physiological result of a general medical condition or a substance, then the diagnosis is one of a psychosis secondary to that condition.[90] Schizophrenia is not diagnosed if symptoms of pervasive developmental disorder are present unless prominent delusions or hallucinations are also present.[90]
Subtypes
With the publication of DSM-5, the APA removed all sub-classifications of schizophrenia.[95] The five sub-classifications included in DSM-IV-TR were:[96][97]
- Paranoid type: Delusions or auditory hallucinations are present, but thought disorder, disorganized behavior, or affective flattening are not. Delusions are persecutory and/or grandiose, but in addition to these, other themes such as jealousy, religiosity, or somatization may also be present. (DSM code 295.3/ICD code F20.0)
- Disorganized type: Named hebephrenic schizophrenia in the ICD. Where thought disorder and flat affect are present together. (DSM code 295.1/ICD code F20.1)
- Catatonic type: The subject may be almost immobile or exhibit agitated, purposeless movement. Symptoms can include catatonic stupor and waxy flexibility. (DSM code 295.2/ICD code F20.2)
- Undifferentiated type: Psychotic symptoms are present but the criteria for paranoid, disorganized, or catatonic types have not been met. (DSM code 295.9/ICD code F20.3)
- Residual type: Where positive symptoms are present at a low intensity only. (DSM code 295.6/ICD code F20.5)
The ICD-10 defines two additional subtypes:[96]
- Post-schizophrenic depression: A depressive episode arising in the aftermath of a schizophrenic illness where some low-level schizophrenic symptoms may still be present. (ICD code F20.4)
- Simple schizophrenia: Insidious and progressive development of prominent negative symptoms with no history of psychotic episodes. (ICD code F20.6)
Sluggish schizophrenia is in the Russian version of the ICD-10. "Sluggish schizophrenia" is in the category of "schizotypal" disorder in section F21 of chapter V.[98]
Differential diagnosis
Psychotic symptoms may be present in several other mental disorders, including bipolar disorder,[99] borderline personality disorder,[100] drug intoxication and drug-induced psychosis. Delusions ("non-bizarre") are also present in delusional disorder, and social withdrawal in social anxiety disorder, avoidant personality disorder and schizotypal personality disorder. Schizotypal personality disorder has symptoms that are similar but less severe than those of schizophrenia.[5] Schizophrenia occurs along with obsessive-compulsive disorder (OCD) considerably more often than could be explained by chance, although it can be difficult to distinguish obsessions that occur in OCD from the delusions of schizophrenia.[101] A few people withdrawing from benzodiazepines experience a severe withdrawal syndrome which may last a long time. It can resemble schizophrenia and be misdiagnosed as such.[102]A more general medical and neurological examination may be needed to rule out medical illnesses which may rarely produce psychotic schizophrenia-like symptoms, such as metabolic disturbance,systemic infection, syphilis, HIV infection, epilepsy, limbic encephalitis, and brain lesions. Stroke, multiple sclerosis, hyperthyroidism, hypothyroidism and dementias such as Alzheimer's disease,Huntington's disease, frontotemporal dementia and Lewy Body dementia may also be associated with schizophrenia-like psychotic symptoms.[103] It may be necessary to rule out a delirium, which can be distinguished by visual hallucinations, acute onset and fluctuating level of consciousness, and indicates an underlying medical illness. Investigations are not generally repeated for relapse unless there is a specific medical indication or possible adverse effects from antipsychotic medication. In children hallucinations must be separated from typical childhood fantasies.[5]Schizophrenia is a severe brain disorder in which people interpret reality abnormally. Schizophrenia may result in some combination of hallucinations, delusions, and extremely disordered thinking and behavior.
Contrary to popular belief, schizophrenia isn't a split personality or multiple personality. The word "schizophrenia" does mean "split mind," but it refers to a disruption of the usual balance of emotions and thinking.
Schizophrenia is a chronic condition, requiring lifelong treatment.In men, schizophrenia symptoms typically start in the early to mid-20s. In women, symptoms typically begin in the late 20s. It's uncommon for children to be diagnosed with schizophrenia and rare for those older than 45.
Schizophrenia involves a range of problems with thinking (cognitive), behavior or emotions. Signs and symptoms may vary, but they reflect an impaired ability to function. Symptoms may include:
- Delusions. These are false beliefs that are not based in reality. For example, you're being harmed or harassed; certain gestures or comments are directed at you; you have exceptional ability or fame; another person is in love with you; a major catastrophe is about to occur; or your body is not functioning properly. Delusions occur in as many as 4 out of 5 people with schizophrenia.
- Hallucinations. These usually involve seeing or hearing things that don't exist. Yet for the person with schizophrenia, they have the full force and impact of a normal experience. Hallucinations can be in any of the senses, but hearing voices is the most common hallucination.
- Disorganized thinking (speech). Disorganized thinking is inferred from disorganized speech. Effective communication can be impaired, and answers to questions may be partially or completely unrelated. Rarely, speech may include putting together meaningless words that can't be understood, sometimes known as word salad.
- Extremely disorganized or abnormal motor behavior.This may show in a number of ways, ranging from childlike silliness to unpredictable agitation. Behavior is not focused on a goal, which makes it hard to perform tasks. Abnormal motor behavior can include resistance to instructions, inappropriate and bizarre posture, a complete lack of response, or useless and excessive movement.
- Negative symptoms. This refers to reduced ability or lack of ability to function normally. For example, the person appears to lack emotion, such as not making eye contact, not changing facial expressions, speaking without inflection or monotone, or not adding hand or head movements that normally provide the emotional emphasis in speech. Also, the person may have a reduced ability to plan or carry out activities, such as decreased talking and neglect of personal hygiene, or have a loss of interest in everyday activities, social withdrawal or a lack of ability to experience pleasure.
Symptoms in teenagers
Schizophrenia symptoms in teenagers are similar to those in adults, but the condition may be more difficult to recognize in this age group. This may be in part because some of the early symptoms of schizophrenia in teenagers are common for typical development during teen years, such as:
- Withdrawal from friends and family
- A drop in performance at school
- Trouble sleeping
- Irritability or depressed mood
- Lack of motivation
Compared with schizophrenia symptoms in adults, teens may be:
- Less likely to have delusions
- More likely to have visual hallucinations
When to see a doctor
People with schizophrenia often lack awareness that their difficulties stem from a mental illness that requires medical attention. So it often falls to family or friends to get them help.
Helping someone who may have schizophrenia
If you think someone you know may have symptoms of schizophrenia, talk to him or her about your concerns. Although you can't force someone to seek professional help, you can offer encouragement and support and help your loved one find a qualified doctor or mental health provider.
If your loved one poses a danger to self or others or can't provide his or her own food, clothing or shelter, you may need to call 911 or other emergency responders for help so that your loved one might be evaluated by a mental health provider. In some cases, emergency hospitalization may be needed. Laws on involuntary commitment for mental health treatment vary by state. You can contact community mental health agencies or police departments in your area for details.
Suicidal thoughts and behavior
Suicidal thoughts and behavior are common among people with schizophrenia. If you have a loved one who is in danger of committing suicide or has made a suicide attempt, make sure someone stays with that person. Call 911 or your local emergency number immediately. Or, if you think you can do so safely, take the person to the nearest hospital emergency room.


.png)

