Blue Circle
Medi Services

A brain arteriovenous malformation (AVM) is a tangle of abnormal blood vessels connecting arteries and veins in the brain.
The arteries are responsible for taking oxygen-rich blood from the heart to the brain. Veins carry the oxygen-depleted blood back to the lungs and heart. A brain AVM disrupts this vital process.
An arteriovenous malformation can develop anywhere in your body but occurs most often in the brain or spine. Even so, brain AVMs are rare and affect less than 1 percent of the population.
The cause of AVMs is not clear. Most people are born with them, but they can occasionally form later in life. They are rarely passed down among families genetically.
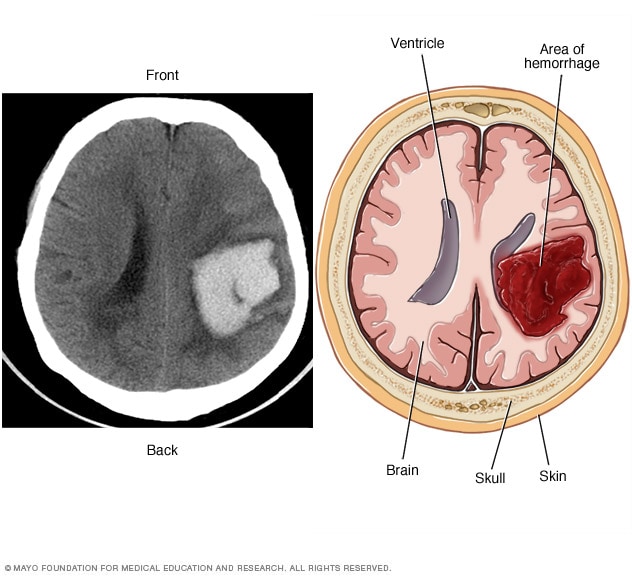
Some people with brain AVMs experience signs and symptoms, such as headache or seizures. AVMs are commonly found after a brain scan for another health issue or after the blood vessels rupture and cause bleeding in the brain (hemorrhage).
Once diagnosed, a brain AVM can often be treated successfully to prevent complications, such as brain damage or stroke.
A brain arteriovenous malformation may not cause any signs or symptoms until the AVM ruptures, resulting in bleeding in the brain (hemorrhage). In about half of all brain AVMs, hemorrhage is the first sign.
But some people with brain AVM may experience signs and symptoms other than bleeding related to the AVM.
In people without hemorrhage, signs and symptoms of a brain AVM may include:
Some people may experience more-serious neurological signs and symptoms, depending on the location of the AVM, including:
Symptoms may begin at any age but usually emerge between ages 10 and 40. Brain AVMs can damage brain tissue over time. The effects slowly build up and often cause symptoms in early adulthood.
Once you reach middle age, however, brain AVMs tend to remain stable and are less likely to cause symptoms.
Some pregnant women may have worsened symptoms due to changes in blood volume and blood pressure.
One severe type of brain AVM, called a vein of Galen defect, causes signs and symptoms that emerge soon or immediately after birth. The major blood vessel involved in this type of brain AVM can cause fluid to build up in the brain and the head to swell. Signs and symptoms include swollen veins that are visible on the scalp, seizures, failure to thrive and congestive heart failure.
Seek immediate medical attention if you notice any signs or symptoms of a brain AVM, such as seizures, headaches or other symptoms. A bleeding brain AVM is life-threatening and requires emergency medical attention.
The cause of brain AVM is unknown, but researchers believe most brain AVMs emerge during fetal development.
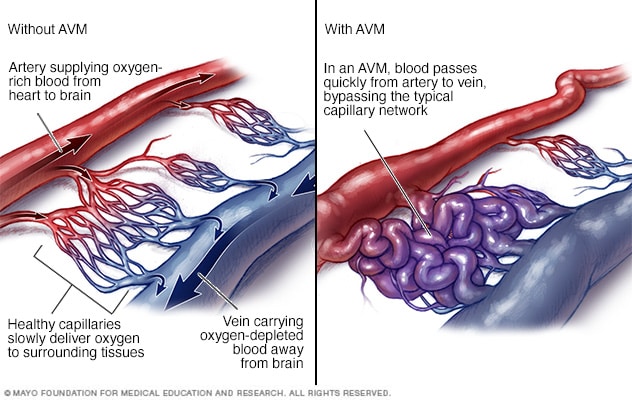
Normally, your heart sends oxygen-rich blood to your brain through arteries. The arteries slow blood flow by passing it through a series of progressively smaller networks of blood vessels, ending with the smallest blood vessels (capillaries). The capillaries slowly deliver oxygen through their thin, porous walls to the surrounding brain tissue.
The oxygen-depleted blood then passes into small blood vessels and then into larger veins that drain the blood from your brain, returning it to your heart and lungs to get more oxygen.
The arteries and veins in an AVM lack this supporting network of smaller blood vessels and capillaries. Instead, the abnormal connection causes blood to flow quickly and directly from your arteries to your veins, bypassing the surrounding tissues.
Anyone can be born with a brain AVM, but these factors may be a risk:
Complications of a brain AVM include:
Bleeding in the brain (hemorrhage).An AVM puts extreme pressure on the walls of the affected arteries and veins, causing them to become thin or weak. This may result in the AVM rupturing and bleeding into the brain (a hemorrhage).
This risk of a brain AVM bleeding ranges around 2 percent each year. The risk of hemorrhage may be higher for certain types of AVMs, or if you have experienced previous AVM ruptures.
Some hemorrhages associated with AVMs go undetected because they cause no major brain damage or symptoms, but potentially life-threatening bleeding episodes may occur.
Brain AVMs account for about 2 percent of all hemorrhagic strokes each year and are often the cause of hemorrhage in children and young adults who experience brain hemorrhage.
Reduced oxygen to brain tissue. With an AVM, blood bypasses the network of capillaries and flows directly from arteries to veins. Blood rushes quickly through the altered path because it isn't slowed down by channels of smaller blood vessels.
Surrounding brain tissues can't easily absorb oxygen from the fast-flowing blood. Without enough oxygen, brain tissues weaken or may die off completely. This results in stroke-like symptoms, such as difficulty speaking, weakness, numbness, vision loss or severe unsteadiness.
Brain damage. As you grow, your body may recruit more arteries to supply blood to the fast-flowing AVM. As a result, some AVMs may get bigger and displace or compress portions of the brain. This may prevent protective fluids from flowing freely around the hemispheres of the brain.
If fluid builds up, it can push brain tissue up against the skull (hydrocephalus).Arteriovenous malformation (AVM) is an abnormal connection between arteries and veins, bypassing the capillary system. This vascular anomaly is widely known because of its occurrence in the central nervous system, but can appear in any location. Although many AVMs are asymptomatic, they can cause intense pain or bleeding or lead to other serious medical problems.
AVMs are usually congenital and belong to the RASopathies. The genetic transmission patterns of AVM, if any, are unknown. AVM is not generally thought to be an inherited disorder, unless in the context of a specific hereditary syndrome.
Symptoms of AVM vary according to the location of the malformation. Roughly 88%[1] of people affected with AVM are asymptomatic; often the malformation is discovered as part of an autopsy or during treatment of an unrelated disorder (called in medicine "an incidental finding"); in rare cases its expansion or a micro-bleed from an AVM in the brain can cause epilepsy, neurological deficit or pain.
The most general symptoms of a cerebral AVM include headache and epilepsy, with more specific symptoms occurring that normally depend on the location of the malformation and the individual. Such possible symptoms include:
Cerebral AVMs may present in a number of ways
In the lungs, pulmonary arteriovenous malformations have no symptoms in up to 29% of cases.
Can occur due to autosomal dominant diseases, such as Hereditary Hemorrhagic Telangiectasia.
In a normal functioning human body, arteries carry blood away from the heart to the lungs or the rest of the body, where the blood passes through capillaries, and veins return the blood to heart. An AVM interferes with this process by forming a direct connection of the arteries and veins. AVMs can cause intense pain and lead to serious medical problems. Although AVMs are often associated with the brain and spinal cord, they can develop in any part of the body.
Arteries and veins are part of the human cardiovascular system. Normally, the arteries in the vascular system carry oxygen-rich blood, except in the case of the pulmonary artery. Structurally, arteries divide and sub-divide repeatedly, eventually forming a sponge-like capillary bed. Blood moves through the capillaries, giving up oxygen and taking up waste products, including CO
2, from the surrounding cells. Capillaries in turn successively join together to form veins that carry blood away. The heart acts to pump blood through arteries and uptake the venous blood.
An AVM lacks the dampening effect of capillaries on the blood flow, which means that the AVM can get progressively larger over time as the amount of blood flowing through it increases, forcing the heart to work harder to keep up with the extra blood flow. It also causes the surrounding area to be deprived of the functions of the capillaries — removal of CO2 and delivery of nutrients to the cells. The resulting tangle of blood vessels, often called a nidus (Latin for "nest"), has no capillaries. It can be extremely fragile and prone to bleeding because of the abnormally direct connections between high-pressure arteries and low-pressure veins. The resultant sign, audible via stethoscope, is a rhythmic, whooshing sound caused by excessively rapid blood flow through the arteries and veins. It has been given the term "bruit", French for noise. On some occasions a patient with a brain AVM may become aware of the noise, which can compromise hearing and interfere with sleep in addition to causing psychological distress.


AVMs are diagnosed primarily by the following methods:
AVMs can occur in various parts of the body:
AVMs may occur in isolation or as a part of another disease (for example, Von Hippel-Lindau disease or hereditary hemorrhagic telangiectasia).
AVMs have been shown to be associated with aortic stenosis.
Bleeding from an AVM can be relatively mild or devastating. It can cause severe and less often fatal strokes. If a cerebral AVM is detected before a stroke occurs, usually the arteries feeding blood into the nidus can be closed off to avert the danger. However, interventional therapy may also be relatively risky.
Normally, arteries carry blood containing oxygen from the heart to the brain, and veins carry blood with less oxygen away from the brain and back to the heart. When an arteriovenous malformation (AVM) occurs, a tangle of blood vessels in the brain or on its surface bypasses normal brain tissue and directly diverts blood from the arteries to the veins.
|
|
Brain AVMs occur in less than 1 percent of the general population. It’s estimated that about one in 200–500 people may have an AVM. AVMs are more common in males than in females.
We don’t know why AVMs occur. Brain AVMs are usually congenital, meaning someone is born with one. But they’re usually not hereditary. People probably don’t inherit an AVM from their parents, and they probably won’t pass one on to their children.
Brain AVMs can occur anywhere within the brain or on its covering. This includes the four major lobes of the front part of the brain (frontal, parietal, temporal, occipital), the back part of the brain (cerebellum), the brainstem, or the ventricles (deep spaces within the brain that produce and circulate the cerebrospinal fluid).
|
Most AVMs don’t grow or change much, although the vessels involved may dilate (widen). Some AVMs may shrink due to clots in part of the AVM. Some may enlarge to redirect blood in adjacent vessels toward an AVM.
Symptoms may vary depending on where the AVM is located:
A brain AVM contains abnormal and, therefore, “weakened” blood vessels that direct blood away from normal brain tissue. These abnormal and weak blood vessels dilate over time. Eventually they may burst from the high pressure of blood flow from the arteries, causing bleeding into the brain.
The chance of a brain AVM bleeding is 1 percent to 3 percent per year. Over 15 years, the total chance of an AVM bleeding into the brain — causing brain damage and stroke — is 25 percent.
The risk of recurrent intracranial bleeding is slightly higher for a short time after the first bleed. In two studies, the risk during the first year after initial bleeding was 6 percent and then dropped to the baseline rate. In another study, the risk of recurrence during the first year was 17.9 percent. The risk of recurrent bleeding may be even higher in the first year after the second bleed and has been reported to be 25 percent during that year. People who are between 11 to 35 years old and who have an AVM are at a slightly higher risk of bleeding.
The risk of death related to each bleed is 10 percent to 15 percent. The chance of permanent brain damage is 20 percent to 30 percent. Each time blood leaks into the brain, normal brain tissue is damaged. This results in loss of normal function, which may be temporary or permanent. Some possible symptoms include arm or leg weakness/paralysis, or difficulty with speech, vision or memory. The amount of brain damage depends on how much blood has leaked from the AVM.
If an AVM bleeds, it can affect one or more normal body functions, depending on the location and extent of the brain injury. Different locations in the brain control different functions:
All blood vessel malformations involving the brain and its surrounding structures are commonly referred to as AVMs. But several types exist:
The best treatment is usually endovascular surgical blocking of the abnormal connections that have caused the fistula. This involves guiding small tubes (catheters) inside the blood vessel with X-ray guidance and blocking off the abnormal connections. Depending on the location and size, many of these can be treated and cured by these less invasive endovascular techniques.
Most AVMs are detected with either a computed tomography (CT) brain scan or a magnetic resonance imaging (MRI) brain scan. These tests are very good at detecting brain AVMs. They also provide information about the location and size of the AVM and whether it may have bled. A doctor may also perform a cerebral angiogram. This test involves inserting a catheter (small tube) through an artery in the leg (groin). Then it’s guided into each of the vessels in the neck going to the brain, and a contrast material (dye) is injected and pictures are taken of all the blood vessels in the brain. For any type of treatment involving an AVM, an angiogram may be needed to better identify the type of AVM.
In general, an AVM may be considered for treatment if it has bled, if it’s in an area of the brain that can be easily treated and if it’s not too large.
It depends on what type it is, the symptoms it may be causing and its location and size.