Blue Circle
Medi Services

Filariasis is a disease group affecting humans and animals, caused by filariae; ie, nematode parasites of the order Filariidae.[1] Of the hundreds of described filarial parasites, only 8 species cause natural infections in humans. The World Health Organization (WHO) has identified lymphatic filariasis as the second leading cause of permanent and long-term disability in the world, after leprosy.
In lymphatic filariasis, repeated episodes of inflammation and lymphedema lead to lymphatic damage, chronic swelling, and elephantiasis of the legs (see the image below), arms, scrotum, vulva, and breasts .[2, 3, 4, 5, 6, 7]
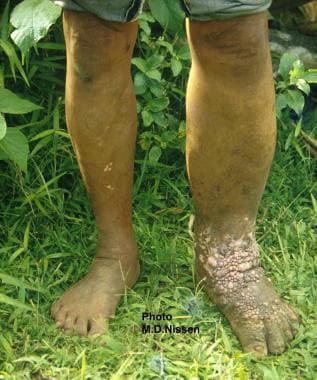
Lymphatic filariasis
The following acute syndromes have been described in filariasis:
Onchocerciasis
The clinical triad of infection in onchocerciasis is as follows:
Loiasis
The diagnostic feature of loiasis is a Calabar swelling, ie, a large, transient area of localized, nonerythematous subcutaneous edema. This is most common around the joints.
Mansonella infections
These are usually asympt omatic. If symptoms are present, they may include fever, pruritus, skin lumps, lymphadenitis, and abdominal pain.
See Clinical Presentation for more detail.
Microfilariae can be detected through examination of the following:
The following imaging studies can be used in the evaluation of filariasis:
Histologic findings include the following:
See Workup for more detail.
Anthelmintics used in the treatment of filariasis include the following:
Surgery
In lymphatic filariasis, large hydroceles and scrotal elephantiasis can be managed with surgical excision. Correcting gross limb elephantiasis with surgery is less successful and may necessitate multiple procedures and skin grafting.
In onchocerciasis, nodulectomy with local anesthetic is a common treatment to reduce skin and eye complications.
Filariasis (or philariasis) is a parasitic disease caused by an infection with roundworms of the Filarioidea type.[1] These are spread by
blood-feeding black flies and mosquitoes. This disease belongs to the group of diseases
called helminthiases.
Eight known filarial nematodes use humans as their definitive
hosts. These are divided into three groups according to the niche within the
body they occupy:
·
Lymphatic filariasis is caused by the worms Wuchereria bancrofti, Brugia malayi, and Brugia timori. These worms occupy the lymphatic system, including the lymph nodes; in chronic cases,
these worms lead to the syndrome of elephantiasis.
·
Subcutaneous
filariasis is caused by Loa loa (the eye worm), Mansonella streptocerca, and Onchocerca volvulus. These worms occupy the subcutaneouslayer of the
skin, in the fat layer. L. loa causes Loa loa filariasis, while O. volvulus causes river blindness.
·
Serous cavity
filariasis is caused by the worms Mansonella perstans and Mansonella ozzardi, which occupy the serous cavity of the abdomen.
The adult worms, which usually stay in one tissue, release early larval forms known as microfilariae into the host's
bloodstream. These circulating microfilariae can be taken up with a blood meal
by the arthropod vector; in the vector, they develop into infective larvae that
can be transmitted to a new host.
Individuals infected by filarial worms may be described as
either "microfilaraemic" or "amicrofilaraemic", depending
on whether microfilariae can be found in their peripheral blood. Filariasis is
diagnosed in microfilaraemic cases primarily through direct observation of
microfilariae in the peripheral blood. Occult filariasis is diagnosed in
amicrofilaraemic cases based on clinical observations and, in some cases, by
finding a circulating antigen in the blood.
The
most spectacular symptom of lymphatic filariasis is elephantiasis—edema with
thickening of the skin and underlying tissues—which was the first disease
discovered to be transmitted by mosquito bites.[2] Elephantiasis results when the parasites
lodge in the lymphatic system.
Elephantiasis affects mainly the lower extremities, while the ears, mucous membranes, and amputation stumps are affected less frequently. However, different species of filarial worms tend to affect different parts of the body; Wuchereria bancrofti can affect the legs, arms, vulva, breasts, and scrotum (causing hydrocele formation), while Brugia timori rarely affects the genitals.[citation needed] Those who develop the chronic stages of elephantiasis are usually amicrofilaraemic, and often have adverse immunological reactions to the microfilariae, as well as the adult worms
The
subcutaneous worms present with rashes, urticarial papules, and arthritis, as well as hyper- and
hypopigmentation macules. Onchocerca
volvulus manifests itself in
the eyes, causing "river blindness" (onchocerciasis), one of the leading causes of
blindness in the world.[citation
needed] Serous
cavity filariasis presents with symptoms similar to subcutaneous filariasis, in
addition to abdominal pain, because these worms are also deep-tissue dwellers.
Human
filarial nematode worms have complicated lifecycles, which primarily consists
of five stages. After the male and female worms mate, the female gives birth to
live microfilariae by the thousands. The microfilariae are taken up by the vector insect (intermediate host) during a
blood meal. In the intermediate host, the microfilariae molt and develop into
third-stage (infective) larvae. Upon taking another blood meal, the vector
insect injects the infectious larvae into the dermis layer of the skin. After
about one year, the larvae molt through two more stages, maturing into the
adult worms.
Filariasis
is usually diagnosed by identifying microfilariae on Giemsa stained, thin and thick blood film
smears, using the "gold standard" known as the finger prick test. The
finger prick test draws blood from the capillaries of the finger tip; larger
veins can be used for blood extraction, but strict windows of the time of day
must be observed. Blood must be drawn at appropriate times, which reflect the
feeding activities of the vector insects. Examples are W. bancrofti, whose vector is a
mosquito; night is the preferred time for blood collection. Loa loa's vector is the deer fly; daytime
collection is preferred. This method of diagnosis is only relevant to
microfilariae that use the blood as transport from the lungs to the skin. Some
filarial worms, such as M.
streptocerca and O. volvulus, produce microfilarae
that do not use the blood; they reside in the skin only. For these worms,
diagnosis relies upon skin snips, and can be carried out at any time.

